
Treatment of Adolescent Idiopathic (Dysplastic) Scoliosis in Patients with Completed Growth (Age >10), with Moderate (20-69°) and Severe (Up to 80-85°) Curvature
Clinical Considerations
Adolescent idiopathic scoliosis (AIS) is characterized by abnormal curvature of the spine, and when it progresses to moderate (20-69°) or severe (up to 80-85°) stages, it leads to significant deformities not only in the spine but also in the rib cage and thoracic cavity. This results in functional disturbances in various body systems, including:
- Central Nervous System (CNS)
- Respiratory system: Compromised lung function due to restricted chest space.
- Cardiovascular system: Altered blood circulation due to compression of the heart.
- Digestive system: Possible digestive issues due to pressure on the abdominal organs.
- Excretory system: Disruptions in kidney function and other organs.
- Endocrine system: Hormonal imbalances related to the spinal deformity and systemic effects.
- Musculoskeletal system: Muscle imbalance and atrophy, joint dysfunction.
Thus, the progression of scoliosis leads to a complex pathological symptom complex, causing it to be recognized not just as a spinal deformity, but as a scoliotic disease that affects the entire body system (A. Radulescu 1961, I.A. Movshovich 1964, Ya.L. Tsivyian 1972, A.I. Kazmin 1980, M.G. Dudin 2005).
Current Treatment Approaches
For adolescents aged 14-16 years with completed growth and mobile spinal deformities, treating moderate (20-69°) and severe (up to 80-85°) scoliosis has become a relatively straightforward task for vertebrology specialists. With the use of modern surgical methods, a full correction can be achieved with high precision.
Optimal Correction Methods for Severe Mobile Scoliosis in Adolescents with Completed Growth
- Dorsal Spinal Release:
- A key technique to release tension in the spine and allow for better realignment of the vertebrae.
- Tenoligamentocapsulotomy (according to Shulutko) is used to facilitate spinal correction by cutting and releasing the tension in spinal ligaments and joint capsules.
- Total Facetectomy:
- Removal of both the upper and lower facet joints to improve mobility and facilitate the alignment of the spine during the correction phase.
- This procedure is essential for mobile deformities to enable full reduction of the curvature.
- Transpedicular Fixation and Posterior Autospinal Fusion:
- Using transpedicular screw systems (CD system) for rigid fixation across the entire length of the deformed spinal segment.
- Thoracoplasty: In some cases, corrective surgery for the rib cage may also be performed to improve chest wall shape and functionality.
- The combination of posterior fusion and screw fixation is considered the most effective method for correcting severe deformities and ensuring stability of the spine after surgery.
These approaches allow for 100% correction of the spinal deformity, achieving excellent long-term results.
Clinical Case Study
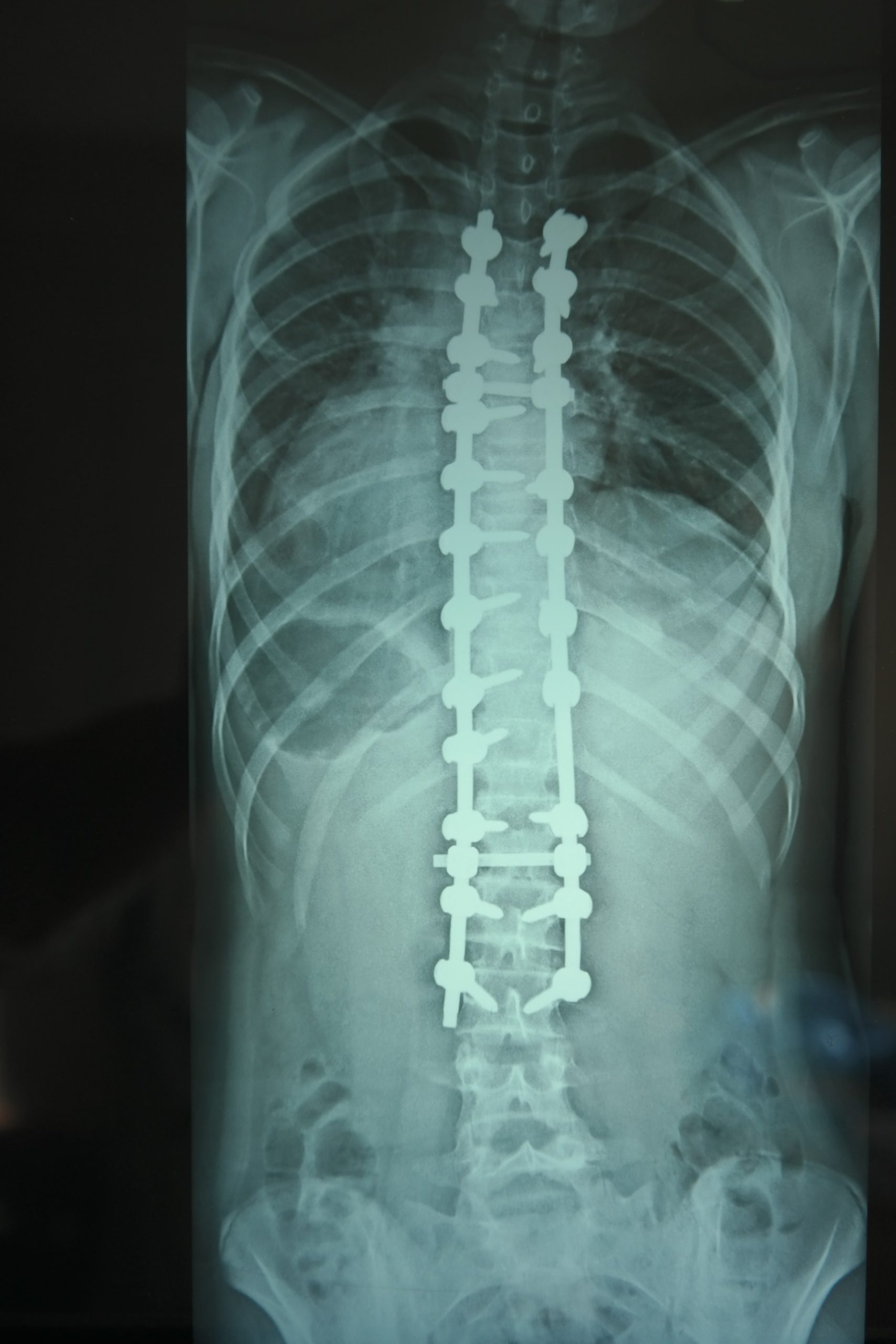
A clinical case of an adolescent with severe idiopathic scoliosis (moderate to severe curve of 70°-80°) was treated using the methods outlined above. The patient underwent:
- Dorsal spinal release via tenoligamentocapsulotomy.
- Total facetectomy (both upper and lower facet joints were removed).
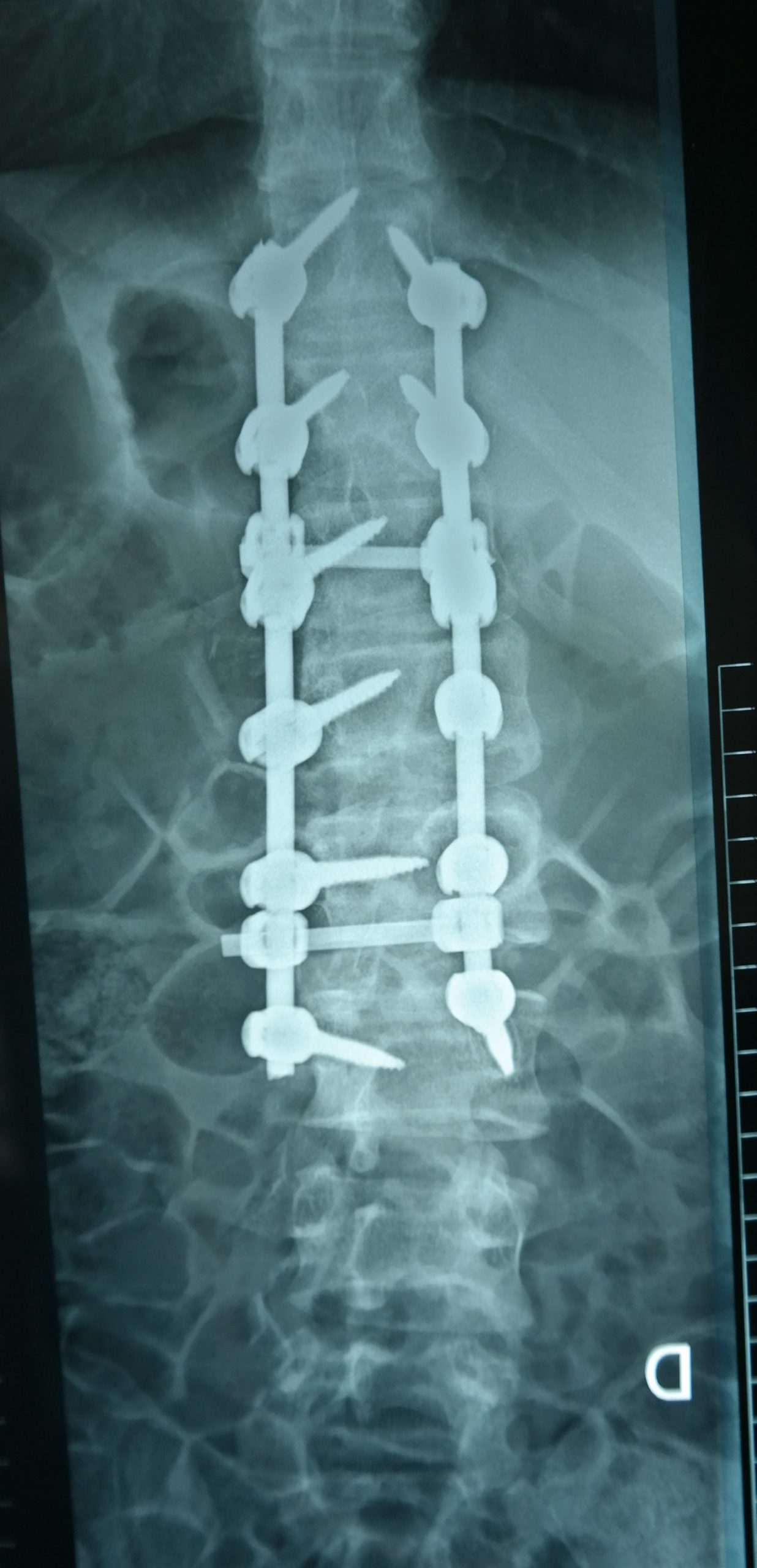
- Transpedicular fixation using a CD system, followed by posterior autospinal fusion.
This approach resulted in a complete correction of the spinal deformity with a significant improvement in posture and function. The patient experienced not only aesthetic improvements but also a marked reduction in pain and better organ function (respiratory and cardiovascular systems) post-surgery.
Key Points:
- Advanced surgical techniques now allow for significant improvement in spinal deformities.
- Full spinal control and stabilization can only be achieved through bilateral fixation (placing two transpedicular screws in each vertebra along the entire curve of the deformity).
- Postoperative recovery: The patient regained full range of motion and was able to return to normal physical activities within a few months, with excellent cosmetic and functional outcomes.
This treatment strategy is recommended for adolescents with severe scoliosis who have completed their growth and present with mobile spinal deformities. The goal is not only to correct the deformity but also to preserve or improve the function of internal organs and overall quality of life.
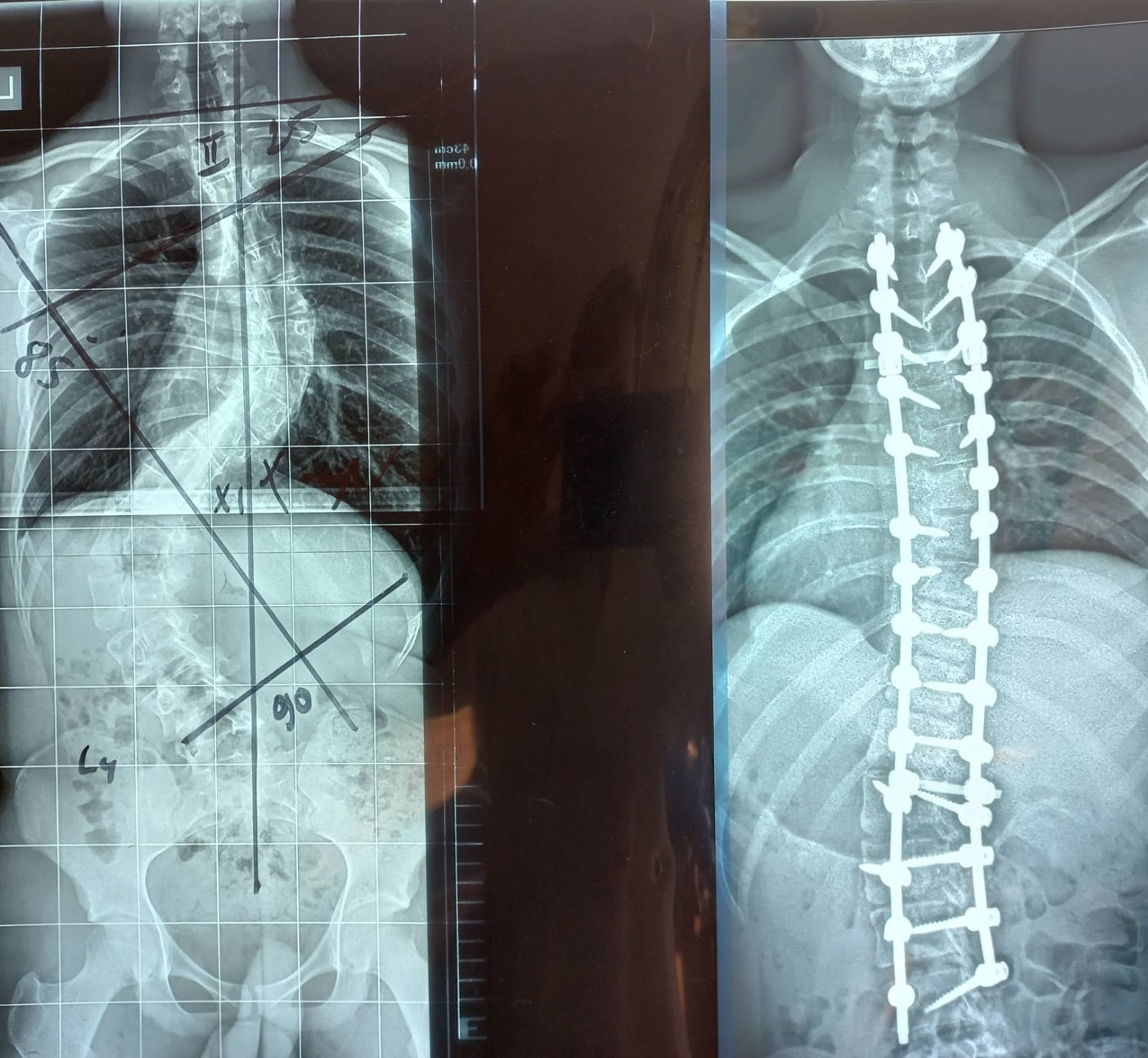
 |  |
Before surgery: Deformation – 78° After surgery: Deformation – 0° Deformation correction: 100% | |
 |  |
Before surgery: Deformation – 78° After surgery: Deformation – 0° Deformation correction: 100% | |